The architecture of data within a healthcare system is the backbone of modern medical care. A robust Entity Relationship Diagram (ERD) ensures that patient information flows securely, accurately, and efficiently across departments. When designing a healthcare database schema, precision is not merely a technical preference; it is a clinical necessity. Errors in data modeling can lead to critical misdiagnoses, billing discrepancies, or compliance violations. This guide details the structural requirements for building a resilient healthcare data model, focusing on integrity, security, and adherence to regulatory standards.
Creating a medical database involves more than simply storing names and dates. It requires a deep understanding of clinical workflows, legal obligations, and the intricate relationships between providers, treatments, and patient histories. This comprehensive overview explores the essential components of healthcare ERD design, ensuring your data infrastructure supports both operational needs and patient safety.
🔍 Foundations of Medical Data Modeling
Before drawing a single line or defining a relationship, one must understand the nature of the data being stored. Healthcare data is distinct due to its sensitivity and the strict regulations governing its use. Unlike e-commerce or social media databases, a healthcare ERD must prioritize data privacy and auditability over sheer transaction speed.
Key characteristics of medical data include:
- High Sensitivity: Information often includes Protected Health Information (PHI), which requires encryption and strict access controls.
- Complex Relationships: A single patient may have multiple providers, multiple treatments, and multiple insurance plans over a lifetime.
- Temporal Variability: Patient conditions change. Historical data must be preserved without corrupting current records.
- Regulatory Constraints: Models must support compliance with laws like HIPAA in the United States or GDPR in Europe.
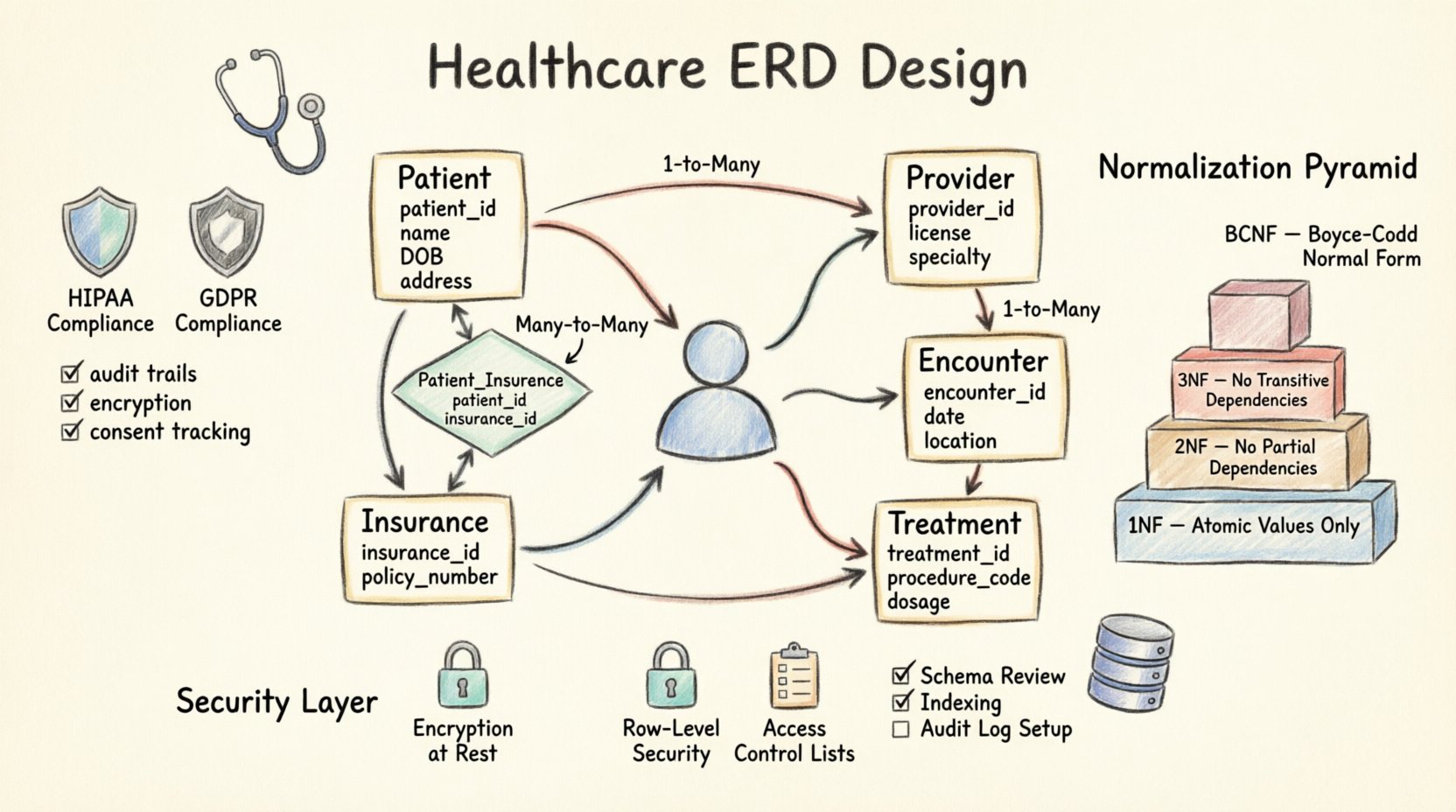
🧩 Core Entities and Attributes
The heart of any healthcare ERD lies in its entities. These represent the tangible or conceptual objects within the system. Below is a breakdown of the primary entities required for a standard patient management system.
| Entity Name | Primary Key | Key Attributes | Compliance Consideration |
|---|---|---|---|
| Patient | patient_id | full_name, DOB, address, gender, emergency_contact | PII Protection, Consent Management |
| Provider | provider_id | license_number, specialty, contact_info, NPI | Credential Verification, Audit Logs |
| Encounter | encounter_id | date, time, location, type, reason_for_visit | Time-stamping, Access Logs |
| Treatment | treatment_id | procedure_code, dosage, start_date, end_date | Precision, Medication History |
| Insurance | insurance_id | provider_name, policy_number, coverage_type | Financial Privacy, Billing Accuracy |
1. The Patient Entity
This is the central anchor of the database. Every other entity typically relates back to a patient record. The patient_id should be a surrogate key (an arbitrary unique identifier) rather than using Social Security Numbers or National Health IDs directly. This practice minimizes the risk of PII exposure in case of a schema leak.
Attributes within this entity must be categorized. Demographic data (name, address) is PII. Clinical data (diagnoses, lab results) is PHI. While both are sensitive, the access rules may differ slightly. For instance, administrative staff may need demographic data but not clinical notes.
2. The Provider Entity
Providers include physicians, nurses, and specialists. Each provider needs a unique identifier to establish accountability. The schema should link providers to their specialties and credentials. This allows for filtering and reporting on care quality by department or individual practitioner.
3. The Encounter Entity
An encounter represents a specific interaction between a patient and the healthcare system. It is the bridge between the patient and the treatment. A single patient can have hundreds of encounters over a lifetime. This entity should store the context of the visit, such as the department visited and the chief complaint.
🔗 Relationships and Cardinality
Defining how entities connect is the most critical step in ERD design. Incorrect cardinality can lead to data redundancy or orphaned records. In healthcare, relationships are often many-to-many, requiring junction tables to resolve.
One-to-Many Relationships
The most common pattern is one patient having many encounters. This is a standard one-to-many relationship. The encounter table holds a foreign key referencing the patient table. This ensures that if a patient record is archived, the historical encounters remain linked.
Many-to-Many Relationships
Consider a provider who treats many patients, and a patient who sees many providers. This is a many-to-many relationship. Directly linking these tables would create ambiguity. Instead, a junction table (often named provider_patient_assignment) is required. This table links the two primary keys and can store additional attributes, such as the date the relationship was established or the role of the provider (e.g., Primary Care Physician vs. Specialist).
Referential Integrity
Referential integrity ensures that relationships remain valid. If a provider leaves the organization, their records should not be deleted immediately. Instead, a status flag (e.g., is_active) should be used. This preserves historical data for auditing and legal purposes without breaking the link in the encounter table.
- Cascading Deletes: Generally discouraged for core entities like
PatientorProvider. - Soft Deletes: Preferred. Mark records as inactive but retain the data.
- Null Handling: Ensure foreign keys cannot be null unless the relationship is truly optional.
🛡️ Compliance and Regulatory Standards
Designing a database without compliance in mind is a liability. The ERD must be built to support the legal frameworks that govern healthcare data. This involves specific design choices that facilitate auditing, consent management, and data minimization.
HIPAA and Data Security
In the United States, the Health Insurance Portability and Accountability Act (HIPAA) sets the standard. While the ERD itself does not implement security, it must support the mechanisms required for compliance.
- Audit Trails: The schema should support a dedicated audit log table. This table records who accessed what data and when. It is linked to the patient or provider tables via foreign keys.
- Data Classification: Columns containing PHI should be clearly named and separated from general administrative data to facilitate targeted encryption strategies.
- Consent Tracking: Include a table to manage patient consent. This links a patient to specific permissions, such as sharing data with a specialist or using data for research.
GDPR and Data Sovereignty
If the system serves European patients, the General Data Protection Regulation (GDPR) applies. This requires a design that supports the “Right to be Forgotten” while maintaining medical necessity.
- Deletion Logic: The model must distinguish between immediate deletion and anonymization. Medical records often require retention for specific periods (e.g., 10 years) even after a patient requests deletion.
- Data Portability: The schema should allow for easy extraction of all data associated with a specific patient ID to fulfill export requests.
🔐 Security Implementation in Schema
Security is not just an add-on; it is a structural element. The database schema dictates how access is controlled.
Encryption at Rest and in Transit
While the ERD defines tables, it influences where encryption is applied. Highly sensitive columns, such as social security numbers or diagnosis codes, should be flagged for encryption. In the design phase, note which fields require this treatment to ensure the database engine supports column-level encryption.
Row-Level Security
Not all users should see all rows. A hospital administrator needs to see billing data for all patients, but a nurse only needs to see records for assigned patients. The ERD should support a user assignment table that links users to specific patient groups or departments. This allows the application layer to filter queries efficiently.
Access Control Lists
Define roles within the schema design. Instead of hardcoding permissions, create a Roles entity and a User_Role junction table. This allows for dynamic permission updates without altering the core medical data tables.
📉 Normalization Strategies
Normalization reduces redundancy and improves data integrity. In healthcare, 3rd Normal Form (3NF) is generally the target, but there are exceptions based on reporting needs.
First Normal Form (1NF)
Ensure atomicity. Each cell in the table should contain a single value. Do not store multiple diagnoses in one column (e.g., “Diabetes, Hypertension”). Instead, create a separate Patient_Diagnosis table. This allows for accurate counting and filtering of specific conditions.
Second Normal Form (2NF)
Ensure all non-key attributes are fully dependent on the primary key. If you have a Provider table, ensure the provider’s specialty is not duplicated in the Encounter table. If a provider changes specialty, it should be updated in one place.
Third Normal Form (3NF)
Ensure no transitive dependencies. If City depends on ZipCode, and ZipCode is in the Patient table, move City to a Location table. This prevents inconsistencies if a city name changes or a zip code is reassigned.
Denormalization for Performance
While normalization is good, healthcare systems often require complex reporting dashboards. In these cases, controlled denormalization may be necessary. For example, a Patient_Summary view might store aggregated data to speed up read operations. However, this data must be recalculated regularly to prevent stale information.
📝 Best Practices for Maintenance and Evolution
A healthcare database is a living system. Patient needs change, and medical codes evolve. The ERD must be designed to accommodate growth without requiring a complete rebuild.
- Versioning: Use version columns for tables that track changes over time. For example, a
Patient_Addresstable should track the validity period (start_date, end_date) rather than updating the row in place. - Standardized Codes: Use external standard codes for medical procedures (e.g., ICD-10, CPT) and medications (e.g., RxNorm). Do not store free text for these fields. This ensures interoperability with other systems.
- Documentation: Maintain a data dictionary. Every column should have a clear description, data type, and business rule. This is vital for onboarding new developers and auditors.
- Archiving Strategy: Plan for data retention. Design separate tables or partitions for historical data that is accessed less frequently. This keeps the active database fast while retaining compliance records.
📋 Checklist for Healthcare ERD Design
Before finalizing the schema, review the following checklist to ensure all critical aspects are covered.
- Data Types: Are dates stored as datetime with timezone awareness?
- Constraints: Are foreign keys enforced to prevent orphaned records?
- Privacy: Are PII fields separated from clinical notes?
- Auditing: Is there a mechanism to track every insert, update, and delete?
- Scalability: Can the schema handle millions of patient records without performance degradation?
- Interoperability: Does the schema support HL7 or FHIR standards for data exchange?
🚀 Implementation Considerations
Once the design is complete, the implementation phase requires careful attention to indexing and query optimization. Healthcare applications are often read-heavy (providers looking up records), but write-heavy during admission and discharge.
- Indexing Strategy: Index foreign keys and search columns. For example, index the
patient_idin theEncountertable to speed up lookup times. Index thelast_nameanddobin thePatienttable for identification. - Transaction Management: Ensure that critical operations, such as prescribing medication, are wrapped in transactions. This guarantees that if one step fails, the entire action is rolled back to prevent partial data entry.
- Backup and Recovery: The schema design should facilitate point-in-time recovery. Consider partitioning tables by date to simplify backup strategies for historical data.
💡 Summary of Key Design Principles
A successful healthcare ERD balances technical efficiency with legal and ethical obligations. By prioritizing data integrity, implementing strict access controls, and adhering to normalization rules, you create a foundation that supports high-quality patient care.
Remember that data is not static. The schema must evolve alongside medical practices. Regular reviews of the ERD against current regulations and clinical workflows are essential. A well-designed model reduces the risk of errors, improves system performance, and ensures that patient trust is maintained through rigorous data stewardship.
Focus on the relationships. Understand the clinical context. Build for compliance first, and performance second. This approach ensures a system that is not only functional but trustworthy.